This transcript has been edited for clarity.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I'm Dr F. Perry Wilson of the Yale School of Medicine.
When I close my eyes and imagine what it is I do for a living, I see a computer screen.
I'm primarily a clinical researcher, so much of what I do is looking at statistical software, or, more recently, writing grant applications. But even when I think of my clinical duties, I see that computer screen.
The reason? The electronic health record (EHR) — the hot, beating heart of medical care in the modern era. Our most powerful tool and our greatest enemy.
The EHR records everything — not just the vital signs and lab values of our patients, not just our notes and billing codes. Everything. Every interaction we have is tracked and can be analyzed. The EHR is basically Sting in the song "Every Breath You Take." Every click you make, it is watching you.
Researchers are leveraging that panopticon to give insight into something we don't talk about frequently: the issue of racial bias in medicine. Is our true nature revealed by our interactions with the EHR?
We're talking about this study in JAMA Network Open.
Researchers leveraged huge amounts of EHR data from two big academic medical centers, Vanderbilt University Medical Center and Northwestern University Medical Center. All told, there are data from nearly 250,000 hospitalizations here.
The researchers created a metric for EHR engagement. Basically, they summed the amount of clicks and other EHR interactions that occurred during the hospitalization, divided by the length of stay in days, to create a sort of average "engagement per day" metric. This number was categorized into four groups: low engagement, medium engagement, high engagement, and very high engagement.

What factors would predict higher engagement? Well, at Vanderbilt there was less engagement with the EHRs of patients who identified as Black, Hispanic, or "other" race. Similar differences were present at Northwestern, except among Black patients who actually got a bit more engagement.
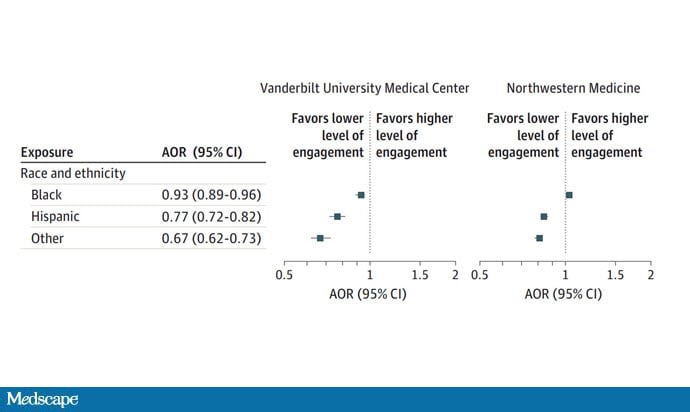
So, right away we need to be concerned about the obvious implications. Less engagement with the EHR may mean lower-quality care, right? Less attention to medical issues. And if that differs systematically by race, that's a problem.
But we need to be careful here, because engagement in the health record is not random. Many factors would lead you to spend more time in one patient's chart vs another. Medical complexity is the most obvious one. The authors did their best to account for this, adjusting for patients' age, sex, insurance status, comorbidity score, and social deprivation index based on their zip code. But notably, they did not account for the acuity of illness during the hospitalization. If individuals identifying as a minority were, all else being equal, less likely to be severely ill by the time they were hospitalized, you might see results like this.
The authors also restrict their analysis to individuals who were discharged alive. I'm not entirely clear why they made this choice. Most people don't die in the hospital; the inpatient mortality rate at most centers is 1%-1.5%. But excluding those patients could potentially bias these results, especially if race is, all else being equal, a predictor of inpatient mortality, as some studies have shown.
But the truth is, these data aren't coming out of nowhere; they don't exist in a vacuum. Numerous studies demonstrate different intensity of care among minority vs nonminority individuals. There is this study, which shows that minority populations are less likely to be placed on the liver transplant waitlist.
There is this study, which found that minority kids with type 1 diabetes were less likely to get insulin pumps than their White counterparts. And this one, which showed that kids with acute appendicitis were less likely to get pain-control medications if they were Black.
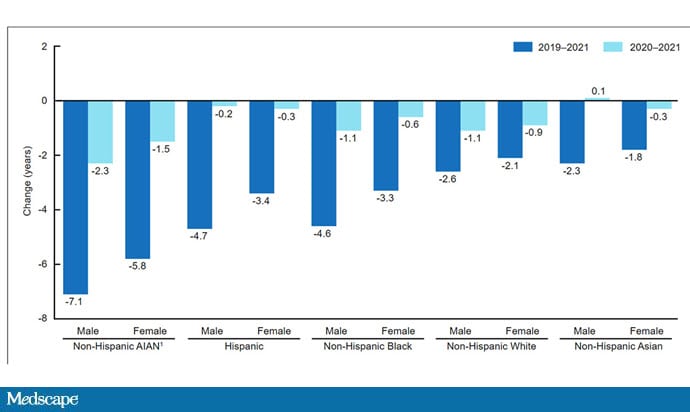
This study shows that although life expectancy decreased across all races during the pandemic, it decreased the most among minority populations.
This list goes on. It's why the CDC has called racism a "fundamental cause of…disease."
So, yes, it is clear that there are racial disparities in healthcare outcomes. It is clear that there are racial disparities in treatments. It is also clear that virtually every physician believes they deliver equitable care. Somewhere, this disconnect arises. Could the actions we take in the EHR reveal the unconscious biases we have? Does the all-seeing eye of the EHR see not only into our brains but into our hearts? And if it can, are we ready to confront what it sees?
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and public health and director of Yale's Clinical and Translational Research Accelerator. His science communication work can be found in the Huffington Post, on NPR, and here on Medscape. He tweets @fperrywilson and his new book, How Medicine Works and When It Doesn't, is available now.
Follow Medscape on Facebook, X (formerly known as Twitter), Instagram, and YouTube
Credits:
Image 1: F. Perry Wilson, MD, MSCE
Image 2: JAMA Network Open
Image 3: Centers for Disease Control and Prevention
Medscape © 2023 WebMD, LLC
Any views expressed above are the author's own and do not necessarily reflect the views of WebMD or Medscape.
Cite this: F. Perry Wilson. Every Click You Make, the EHR Is Watching You - Medscape - Oct 11, 2023.





Comments